Vascular Dysfunction: A Deeper Look
The second of the three pathways: when blood and oxygen aren't reaching the optic nerve when they need to, even at normal pressure.
The second of the three pathways covered in The Ratchet Effect is vascular dysfunction — the part of the picture where damage occurs not because pressure is too high, but because blood and oxygen aren't reaching the optic nerve when they need to. It's the pathway that explains why some people develop glaucoma damage at completely normal eye pressure, and why others, even with well-controlled pressure, continue to progress.
This article goes deeper on what vascular dysfunction actually is, what causes it, what you can influence, and what to watch for.
What "vascular dysregulation" actually means
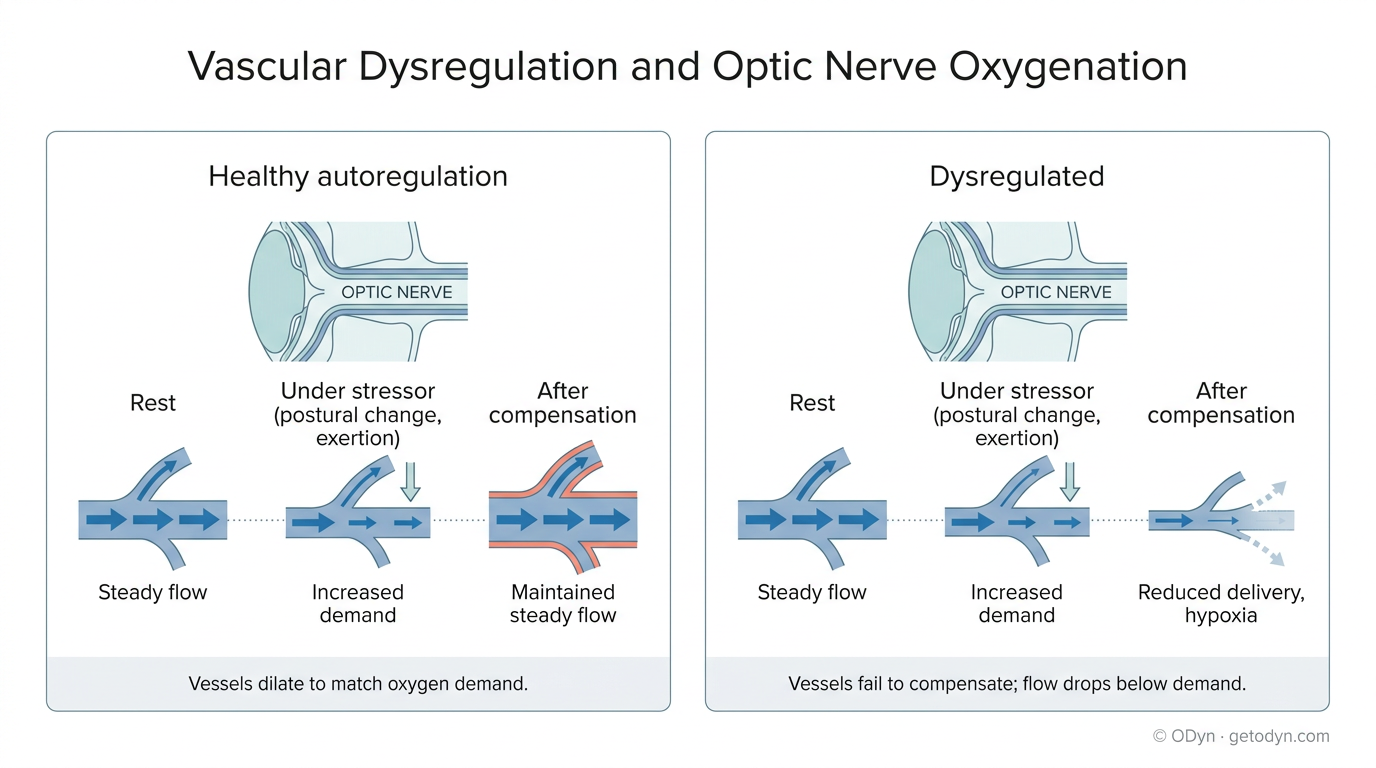
Healthy blood vessels do something quietly impressive — they constantly adjust their diameter to maintain steady blood flow despite shifting demands. When you stand up, vessels in your eyes have to compensate for the drop in head-level blood pressure. When you exercise, oxygen demand increases and vessels widen to deliver more. When systemic blood pressure spikes or drops, ocular vessels adjust to keep flow at the optic nerve relatively constant. This dynamic balancing act is called autoregulation.
When autoregulation works, the optic nerve gets the oxygen it needs through whatever the body is doing. When autoregulation fails or weakens, the optic nerve becomes vulnerable — flow drops out of sync with demand, brief hypoxic episodes occur, and over time those episodes leave damage behind.
That failure has a name in the research literature: vascular dysregulation. And it's now well-established as a contributing factor in glaucomatous damage, particularly in patients whose pressure measurements look unremarkable.
Two ways it shows up
Vascular dysregulation generally falls into one of two categories.
Primary vascular dysregulation is constitutional — it's the way some people's vascular systems are wired from birth. People with this predisposition tend to have a cluster of related signs: cold hands and feet, low blood pressure, heightened sensitivity to cold or stress, sometimes migraine, sometimes tinnitus. The body's vascular response to stimuli is amplified or unstable. In the ophthalmology world, this constellation is often referred to as Flammer syndrome, named after the Swiss researcher who first connected it to glaucoma. A meaningful portion of patients with normal-tension glaucoma have this underlying constitution.
Secondary vascular dysregulation is acquired. It can develop from systemic disease (atherosclerosis, diabetes), from the vascular changes that come with aging, or from prior structural damage to the optic nerve vasculature itself — which is what we covered in the Ratchet Effect's scenario, where a prolonged pressure spike deformed the vessels and impaired their ability to flex.
The two types matter in different ways. Primary dysregulation is something you live with and manage. Secondary dysregulation is something you can accumulate, and prevention of further accumulation is meaningful.
Why it's one of the three pathways
Recall the framing from The Ratchet Effect: oxygen availability to the optic nerve is the root variable; pressure spikes, vascular dysregulation, and altitude are three distinct ways that supply gets disrupted.
In the pressure pathway, IOP is the active variable interrupting oxygen delivery. In the vascular pathway, pressure may be entirely normal. The disruption comes from the delivery system itself — vessels that can't compensate, vessels that constrict when they should dilate, vessels that fail to ramp up flow when demand increases. The result at the cellular level is the same: retinal ganglion cells starved of oxygen, micro-damage that accumulates, blind spots that grow over time.
This is why some glaucoma genuinely does progress at low pressure. As we discussed in the previous article, it's not that the normal-tension diagnosis is always wrong — it's that for some patients, the pressure really is steady and unremarkable, and damage is being driven primarily by what's happening in the vasculature rather than what's happening in the pressure.
What you can influence
Vascular dysregulation is harder to address directly than dietary spike triggers, and we want to be honest about that.
The constitutional element — primary vascular dysregulation, Flammer syndrome territory — isn't something you eliminate. It's something you work with. Researchers in this area have had clinical experience using calcium channel blockers and magnesium supplementation as supportive interventions, both of which require physician oversight. Lifestyle factors that support overall vascular health — adequate hydration, avoiding extreme cold exposure when possible, maintaining a healthy weight, not being underweight — also matter, but their individual effect sizes are modest.
The acquired element is partly preventable. The single biggest lever, in our view, is preventing the kinds of pressure events that cause secondary vascular damage in the first place — which loops back to the importance of identifying and stopping spike triggers, and to the value of home tonometry that makes those triggers visible.
The substance-related element is where most users have the most direct daily control, and it's also where there are the most surprising effects.
Substances with vascular effects
Many things you put into your body have vascular effects you may not be aware of. A partial list:
- Caffeine is a vasoconstrictor — it temporarily reduces blood flow in many vascular beds, including ocular ones, while also modestly raising eye pressure in some people.
- Nicotine is a vasoconstrictor.
- Decongestants containing pseudoephedrine or phenylephrine constrict blood vessels.
- Some prescription medications have vasoactive properties as primary or side effects, including beta-blockers, calcium channel blockers, and certain antidepressants.
- Various supplements marketed for circulation, energy, or cognitive performance act on the vascular system, sometimes in ways that are less predictable than their marketing suggests.
The key word in that list is unpredictable. Most of these substances have an average effect that can be characterized in the research literature. But individual responses vary considerably. Two people taking the same dose of the same substance can have meaningfully different vascular responses based on their underlying constitution, other medications, age, hydration, and factors that aren't fully understood.
The case of ginkgo biloba
Ginkgo biloba deserves a closer look because it sits at an intersection that many glaucoma patients encounter.
It's commonly recommended for circulation, and within ophthalmology specifically, several studies have suggested it can increase ocular blood flow and produce modest visual field improvements in some patients with normal-tension glaucoma. On the surface, that looks like a good fit for the vascular pathway — a substance that improves blood flow being given to patients whose problem is reduced blood flow.
The picture is more complicated than that.
First, ginkgo has anti-platelet effects. It interferes with normal blood clotting, which is part of how it influences circulation. The trade-off is increased bleeding risk, including documented case reports of bleeding events in and around the eye. For the optic nerve specifically, micro-hemorrhages — small leaks in the vasculature — can reduce effective blood supply rather than improve it.
Second, individual responses vary substantially. Published studies report group averages, but within any given study population there are patients who improve, patients who show no measurable change, and patients who experience symptoms or vision changes consistent with a negative response. Anecdotal reports from patients include both positive subjective experiences and reports of new visual symptoms following ginkgo use.
Third, the systemic vasodilation ginkgo produces doesn't map predictably onto optic nerve perfusion. The body's overall vascular response can, in some individuals, redirect blood flow in ways that don't favor the optic nerve, even when measured ocular blood flow appears to increase on average.
We are not saying ginkgo is dangerous, and we are not saying it never helps. The honest reading of the evidence is that it sometimes helps, sometimes doesn't, sometimes appears to worsen things, and there is no reliable way to predict which category any individual patient will fall into without observing what actually happens.
That last sentence is the central message of this article, applied to a specific substance. With anything that has vascular effects, you cannot assume the average research finding applies to you. The only way to know what something is doing to your optic nerve perfusion is to monitor — eye pressure changes if they occur, but also subjective vision symptoms, and ideally formal testing if you and your ophthalmologist can establish a baseline and track from it.
If you have been taking ginkgo or are considering it, that's worth a conversation with your ophthalmologist, paired with a plan for monitoring whether it is helping or hurting your specific situation.
What to watch for
Vascular dysregulation often doesn't announce itself with the kind of clear pressure signal a dietary IOP trigger does. The signs are subtler and easier to dismiss:
- Visual changes during or after exertion, particularly large-muscle exertion
- Visual changes when moving from warm to cold environments
- Visual changes after standing up quickly, especially first thing in the morning
- A sense that vision in one or both eyes "comes and goes" in a way that's distinct from floaters
- New blurring that wasn't there before, particularly across broader areas of the visual field rather than localized spots
We cover these signs in detail in the upcoming article on Recognizing Optic Nerve Distress. The point here is that the vascular pathway often shows up first in patterns of subjective vision change rather than in numbers on a tonometer reading.
What this connects to
The third pathway covered in The Ratchet Effect — altitude — is also a vascular story in many ways. Lower oxygen availability and reduced atmospheric pressure both stress the vascular system that's trying to keep your optic nerve oxygenated. People with vascular dysregulation are particularly affected by altitude, because the underlying system is already operating with less margin.
If vascular dysfunction is part of your picture, the altitude article will be especially relevant. So will the article on Recognizing Optic Nerve Distress, which translates the abstract concept of "compromised perfusion" into the concrete signs you can observe in your own daily life.