IOP Diurnal Fluctuation: The Full Picture
Eye pressure isn't a single number — it's a curve. Understanding what's normal fluctuation, what's a spike, and what causes the difference is the foundation of self-management.
When most people think about their eye pressure, they think about a single number. The number their doctor told them. Maybe 14, maybe 18. Whatever it was, it became their pressure — the way they describe their condition to themselves and to others.
That number doesn't really exist.
Your eye pressure isn't one number. It's a curve. A constantly moving line that rises and falls throughout every hour of every day. The number on your chart is just one point on that line — captured at one moment, in one chair, in one office.
To manage glaucoma well, you have to understand what the rest of that line looks like.
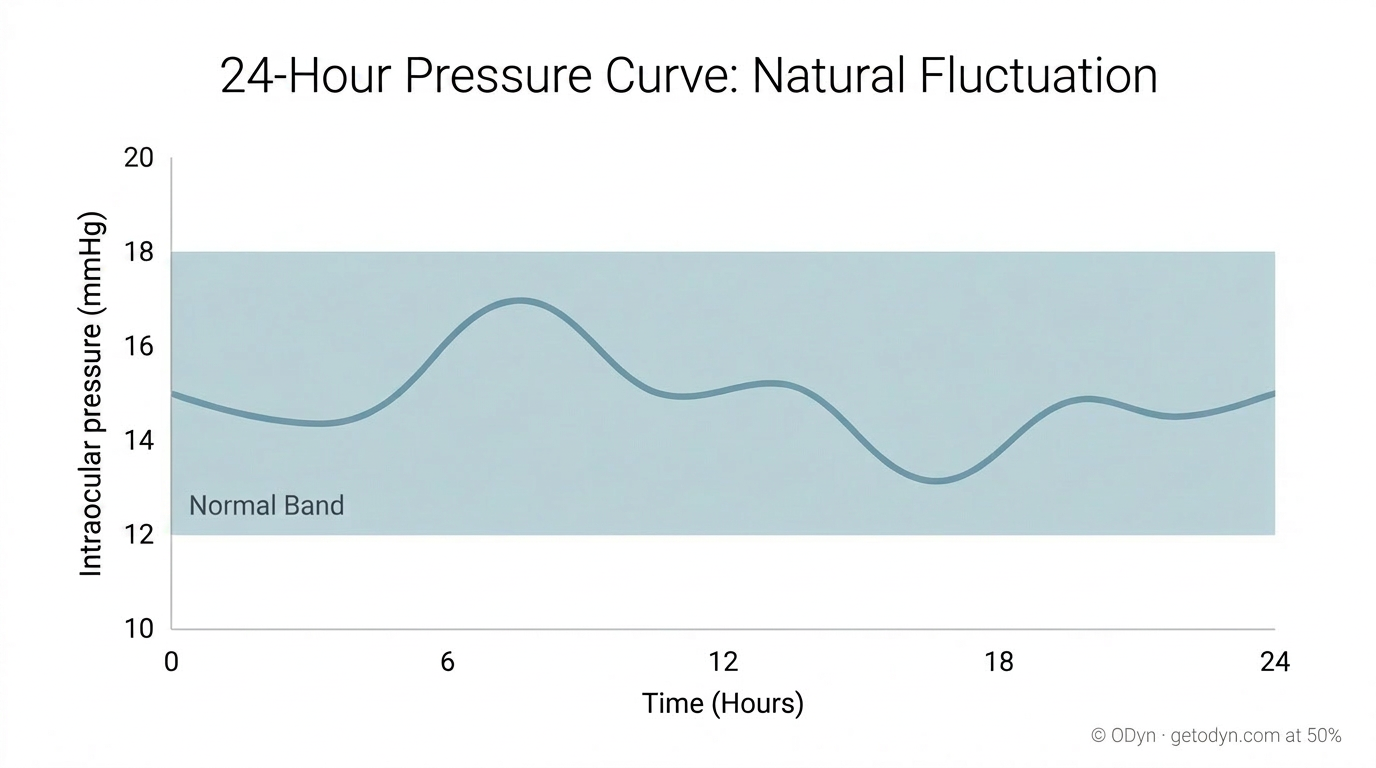
What's normal
In a healthy eye, pressure fluctuates throughout the day, typically by something on the order of three to five points above and below your average. This isn't a problem. It's expected. Your pressure naturally drifts higher in the early morning hours, often peaks shortly after waking, and tends to settle lower in the late afternoon and evening. There are physiological reasons for this — changes in body position, fluid dynamics, hormonal cycles. The fluctuations themselves don't drive damage. They're part of how the system works.
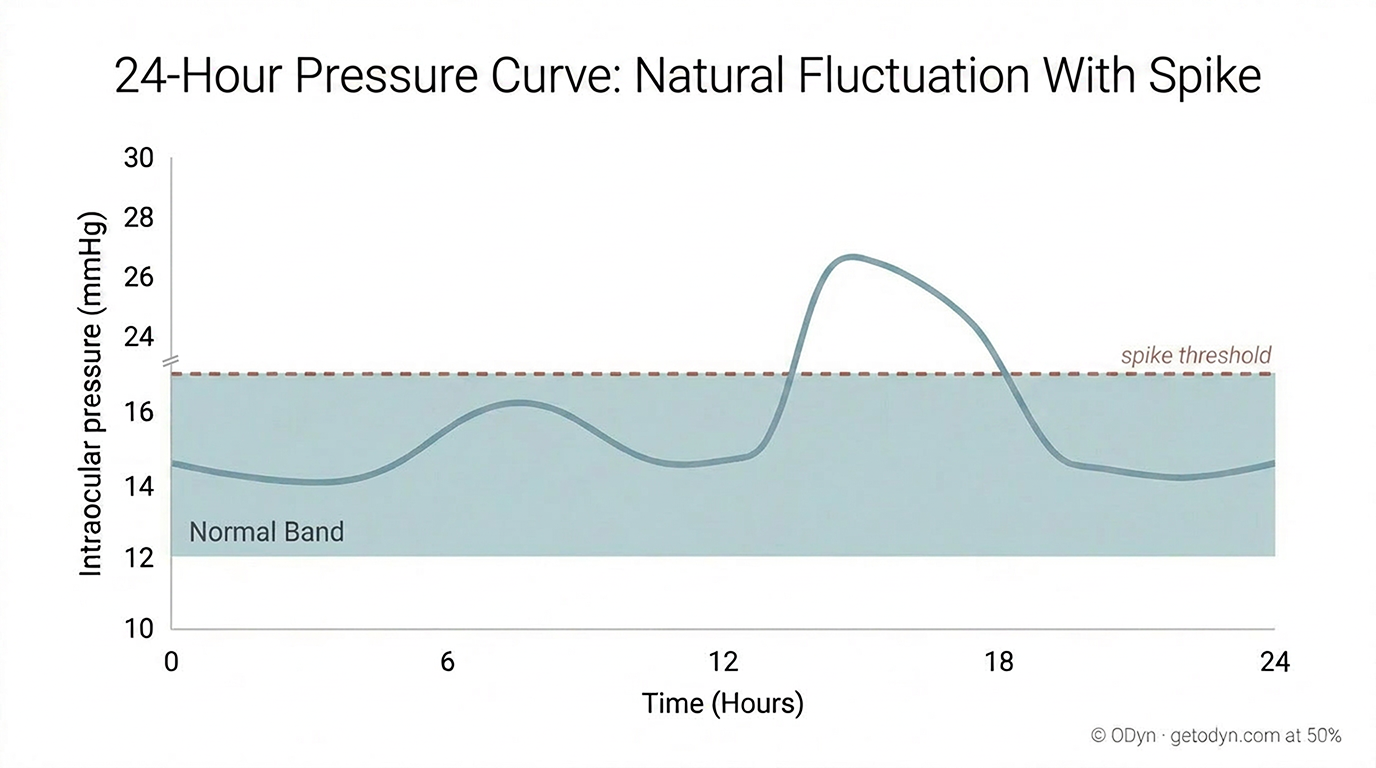
The trouble starts when something pushes pressure outside that normal range.
What a spike is
A spike is what happens when your pressure jumps significantly above its usual range and holds there for a meaningful period — often several hours, sometimes longer. We're not talking about a one-point bump. We're talking about something that pushes pressure 8, 10, 15 points or more above your baseline. That's the territory where damage starts to accumulate.
Here's the part that surprises people. A spike doesn't have to last for days to cause harm. It doesn't even have to last a full day. A few hours, repeated over time, is often enough. The retinal ganglion cells we discussed in the first piece — the ones that don't grow back — start losing oxygen supply when pressure stays elevated long enough to compress the small blood vessels feeding them. That window is measured in hours, not weeks.
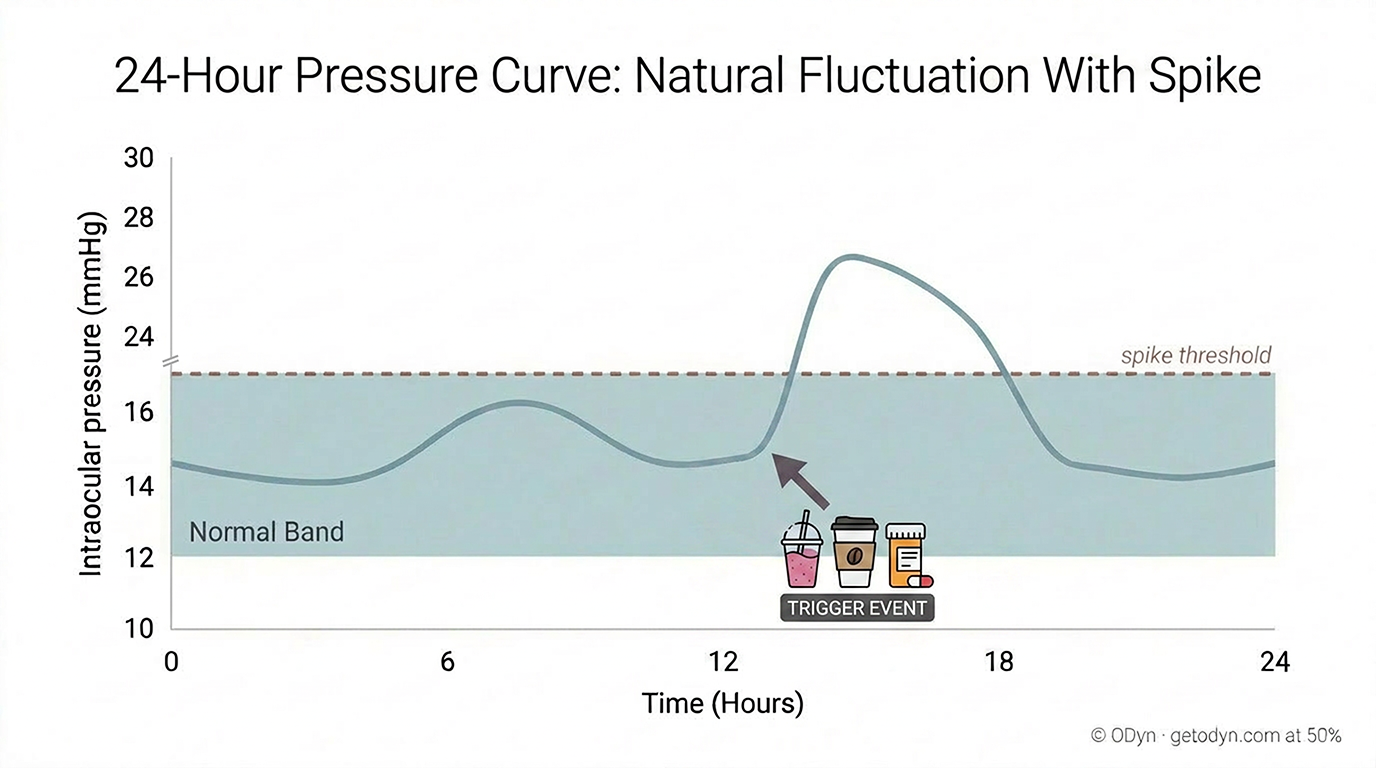
Spikes have causes
For most people who experience these spikes, they're not random. They have causes. Specific, identifiable, often controllable causes. Something you ate. Something you drank. A medication you started. A supplement someone recommended. The body's response to that input pushes pressure up, holds it there for a few hours, and then it gradually returns to baseline as the substance is metabolized and cleared.
If that's happening to you on a regular basis, and you don't know about it, you are progressing your own glaucoma — without ever realizing it.
That's the part we want you to sit with for a moment.
It's not the genetics. It's not bad luck. It's not unavoidable disease progression. It's something you're doing, probably daily, that you could simply stop doing if you knew it was the cause. The action is small. The behavior is changeable. The cost of stopping is essentially nothing. But the consequence of not knowing is permanent vision loss.
Why standard care has limited power here
This is, in our view, the most important and most under-communicated reality of glaucoma management.
It's also the reason the standard model of care — quarterly visits with single-point measurements — has such limited power to prevent progression. A doctor who sees you for fifteen minutes every three months, taking one or two readings at one time of day, has almost no ability to identify what's spiking your pressure between visits. They're working with four data points a year. The events they're trying to prevent are happening in the gaps.
What's actually uncontrollable vs. controllable
Not every fluctuation is a spike, and not every spike is dietary. There are genuinely uncontrollable factors that influence pressure — stress, sleep quality, body position during sleep, certain medications you can't simply stop taking. These all matter to some degree. But based on what continuous monitoring research consistently shows, the major drivers of damaging spikes — the ones that produce 10, 15, 20-point excursions for hours at a time — are usually controllable. They're usually something the person introduced into their daily routine without realizing it would matter.
What to do with this
The starting point is the same conclusion the previous piece arrived at. You need data. Not four data points a year, but enough readings, taken often enough, that the actual shape of your pressure curve becomes visible. Your baseline. Your typical daily pattern. And critically, the events that fall outside that pattern — the spikes that quarterly visits will never catch.
Once you can see your curve, the next step is connecting the events on it to the choices you're making in your day. That's the work the rest of this section is built to support — identifying triggers, isolating causes, and turning what looks like random progression into something you can actually control.
The single number on your chart is a starting point. But it isn't your pressure. The whole curve is your pressure. And once you can see it, almost everything about how you manage this disease changes.