Altitude and Oxygen Availability
The third pathway: what altitude actually does to oxygen availability, how it affects the optic nerve, and the practical difference between visiting and living high.
The third pathway covered in The Ratchet Effect is altitude — the part of the picture where the air itself contains less of what your optic nerve needs. Of the three pathways, this one is often the most overlooked, partly because its effects are spread out over hours and days rather than concentrated in a single dramatic event, and partly because most patients aren't told to think about it at all. This article goes deeper on what altitude actually does to oxygen availability, how it affects the optic nerve, and what the practical implications are for visiting versus living at higher elevations.
Two things change as altitude rises
The percentage of oxygen in the air itself stays remarkably constant — roughly 21% at every elevation on Earth. What changes is the air itself, and how much oxygen ends up reaching your bloodstream.
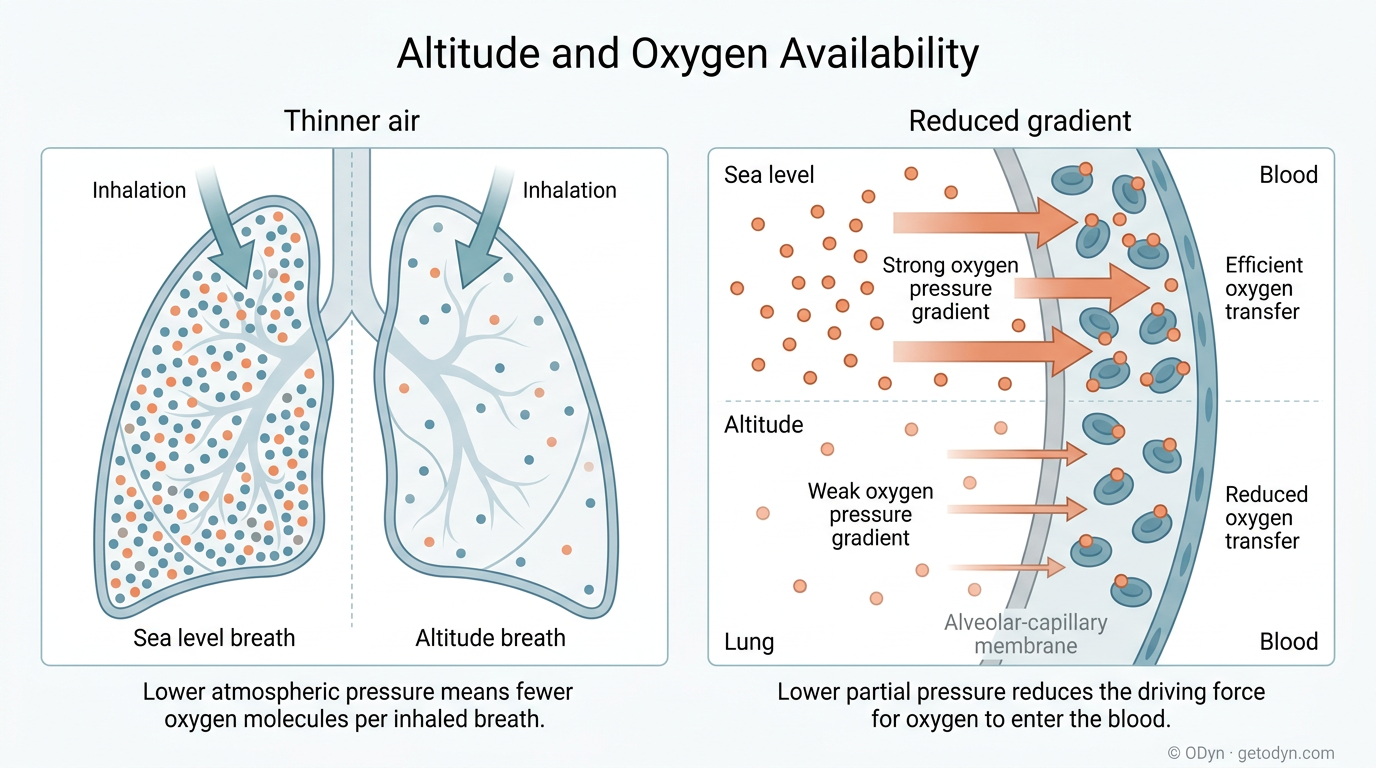
The air becomes thinner. At higher elevations, atmospheric pressure is lower and the air is less dense — there are fewer total molecules per unit volume. Oxygen still makes up about 21% of the air, but a single breath at altitude contains fewer molecules overall, and therefore fewer oxygen molecules in absolute terms, than the same breath at sea level. This is why altitude is sometimes described as a hypobaric environment.
Oxygen transfers less efficiently into your blood. The lower air pressure also reduces how effectively oxygen moves from your lungs into your bloodstream. At sea level, the high partial pressure of oxygen drives a strong gradient that pushes oxygen across the lung membrane and into your blood. At altitude, that gradient is weaker, and even the oxygen that does reach your lungs is absorbed less efficiently.
These two effects compound. Less oxygen entering your lungs per breath, and less efficient transfer of what does enter — together they meaningfully reduce the oxygen reaching every oxygen-dependent process in your body, including the supply to your optic nerve. For practical scale: in Denver, at about 5,280 feet (1,610 m), you receive roughly 82–85% of the oxygen per breath that you would at sea level. At 10,000 feet (3,000 m), you receive about 70% of sea-level oxygen.
Three altitude bands worth thinking about
Altitude effects intensify gradually rather than switching on at sharp thresholds, but in practice there are three rough zones where the experience starts to feel meaningfully different:
Sea level to roughly 4,000 feet (1,200 m). This is the baseline most physiology research is calibrated to. Most healthy people have no measurable systemic effects at these elevations. From a glaucoma perspective, this zone is generally not a concern in itself.
4,000 feet (1,200 m) up to 7,000 feet (2,100 m). This is moderate altitude territory. Most healthy people adapt within days, but oxygen availability is meaningfully lower, baseline blood oxygen saturation is reduced, and exertion produces larger oxygen deficits than it would at sea level. People with vascular dysregulation or recent damage feel this range more than the average person does.
Above 7,000 feet (2,100 m). This is high altitude. Oxygen availability is significantly lower, baseline saturation drops further, and the body's compensatory mechanisms are working harder all the time. In this range, however, the body typically operates in a state of compensated hypoxia — while the system works harder during the day, it is still generally able to absorb enough oxygen overnight to recharge its cellular ATP "battery."
The 10,000-foot cliff. Rather than a soft sub-distinction, 10,000 feet (3,000 m) represents a precise physiological cliff. At exactly this elevation, the arterial partial pressure of oxygen (pO2) hits roughly 60 mmHg, pushing the body into uncompensated hypoxia. At this point, the system operates at a daily net loss because it can no longer fully recharge its ATP stores overnight. We explore this hard mathematical limit in depth in The 10,000-Foot Cliff.
What this looks like in your blood oxygen
A finger or wrist pulse oximeter shows you SpO2 — the percentage of your hemoglobin currently carrying oxygen. This number gives you a useful, immediate read on the oxygen story at your specific elevation.
Approximate resting baselines for healthy adults:
- Sea level: typically 97–100%
- Moderate altitude (4,000–7,000 feet, 1,200–2,100 m): around 94–95%
- 7,000–9,000 feet (2,100–2,700 m): around 91%, sometimes lower
- 10,000 feet (3,000 m) and above: around 89% or lower is not unusual
Exertion changes the picture in a way that matters more for glaucoma than the resting numbers alone. At moderate altitude, moderate exertion can sometimes pull SpO2 down by 5 to 10 points, and at high altitude, that drop can be steeper still. The result is a kind of double hit: at altitude, you start with a lower baseline, and exertion pulls you further from that baseline than the same exertion would at sea level.
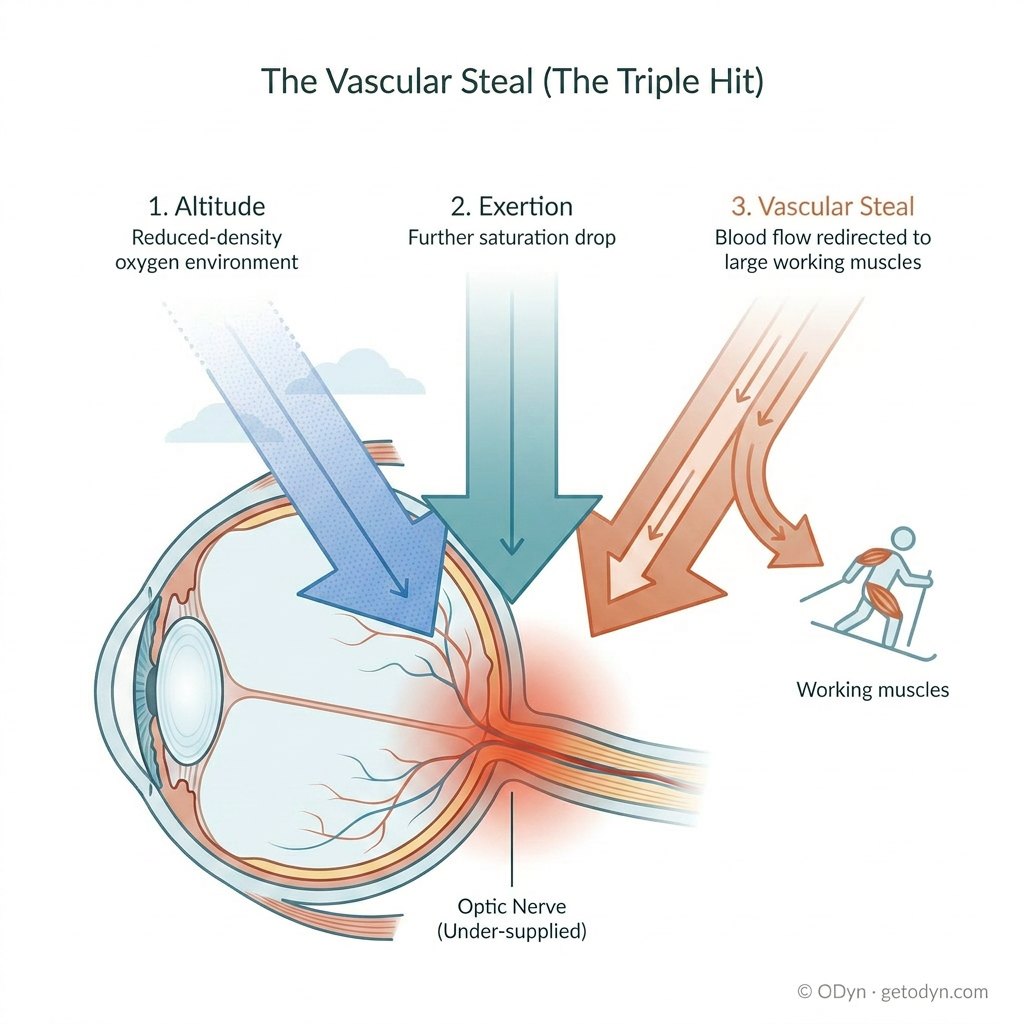
The vascular steal (the triple hit). When that altitude exertion involves large muscle groups — skiing, snowboarding, hiking, climbing — a third compounding effect kicks in. Working muscles demand a large share of cardiac output, and the body redistributes blood flow accordingly: vessels in the working muscles dilate, and flow to non-prioritized systems, including the optic nerve, is reduced. So the optic nerve loses on three fronts at once: a lower baseline oxygen supply (altitude), reduced saturation under exertion (the double hit), and a smaller share of what blood does flow (the vascular steal). Each effect alone is manageable for a healthy system; together, in a system with already-compromised autoregulation, they can push the optic nerve into the kind of distress event covered in Recognizing Optic Nerve Distress.
Why this matters for the optic nerve specifically
A perfectly healthy optic nerve, with healthy autoregulation, can compensate for moderate reductions in oxygen availability. A compromised system has less margin to work with. The compromised vessels can't ramp up oxygen delivery the way healthy vessels would. Exertion that would have been tolerated at sea level now drives the eye into a hypoxic state. Each episode is small, but the damage compounds over time. Altitude rarely causes glaucoma damage on its own in healthy individuals; what it does is expose and amplify whatever vulnerability already exists.
Visiting versus living: the most important practical distinction
One of the most consequential questions for glaucoma patients is whether occasional altitude exposure should be treated as a serious concern. The honest answer is that it depends on what you mean by exposure.
Visiting altitude — day visits and short multi-day stays — is manageable for most early-stage and many moderate-stage patients with awareness and monitoring. The exposure is bounded; the system has time to recover; the cumulative effect is small. Pay attention to symptoms during exertion, take altitude-related fatigue or visual disturbance seriously when they show up, and you can keep skiing trips, mountain visits, and high-elevation travel as part of a reasonable life.
Living at altitude is a fundamentally different situation. Here, the damage on any given day may be nano-level — but it accumulates continuously over years, leading to a capacity crisis characterized by cumulative metabolic debt. You aren't just overtaxing the system; you are severely depleting the cellular energy reservoir over time. While this mitochondrial drain can eventually be reversed in an oxygen-rich environment, chronic hypoxic stress risks permanent structural losses, such as dead cells and collapsed micro-capillaries.
Years add up. A patient who would have weathered a few weeks of exposure without noticeable change can experience meaningful progression after several years of continuous residence at the same altitude. For a detailed breakdown of how living above 10,000 feet (3,000 m) depletes cellular energy reserves and alters your microvascular baseline over time, see The 10,000-Foot Cliff.
This distinction shapes how to think about altitude as a glaucoma patient at different stages.
- Early stage. Occasional high altitude exposure across the 7,000–9,900 ft (2,100–3,000 m) range is manageable with awareness and monitoring. Long-term residence at higher elevations is worth a careful look — if you have flexibility about where you live, that flexibility is worth keeping. Where long-term residence at high altitude is a must, aim for the lower end of the range if possible; the difference between 7,500 ft (2,300 m) and 9,500 ft (2,900 m) is meaningful in cumulative metabolic terms. Long-term residence at or above 10,000 ft (3,000 m) is not advisable for glaucoma patients at any stage, given the physiology covered in The 10,000-Foot Cliff.
- Moderate stage. Visits remain workable, but pay close attention to optic nerve distress symptoms during exertion and stop the exertion if symptoms appear. Long-term residence at high altitude (7,000–9,900 ft / 2,100–3,000 m) warrants more active consideration — the metabolic margin available at this stage is narrower than earlier in the disease.
- Advanced stage. All high-altitude exposure deserves serious risk-benefit consideration. Long-term residence above moderate altitude (above 7,000 ft / 2,100 m) is the kind of decision worth examining honestly with your ophthalmologist, given how much reserve has already been lost.
For people in the 4,000–7,000 ft (1,200–2,100 m) range — a band that includes a meaningful portion of the U.S. population, residents of major international cities, and many others worldwide — the right posture is awareness and monitoring rather than alarm. Establish your baseline SpO2, track it periodically, and watch for optic nerve distress symptoms during exertion. If you don't have symptoms, that's good information. If you do, take it seriously and consider what it implies about your specific situation.
What to do
A few practical points anyone with glaucoma at altitude can act on:
- Know your baseline SpO2. A finger or wrist oximeter establishes what's normal for you at your altitude.
- Monitor during exertion. SpO2 measurements during and after physical activity tell you how your system responds to demand.
- Watch for optic nerve distress symptoms during exertion, particularly large-muscle exertion like skiing, hiking, or carrying heavy loads.
- For proactive monitoring at altitude, consider advanced telemetry. The PERG, contrast sensitivity, and nocturnal oximetry triad — detailed in The 10,000-Foot Cliff — surfaces metabolic and functional deficits before they translate into permanent loss.
- Consider supplemental oxygen as a buffer, particularly for residence at moderate-to-high altitudes or for prolonged exertion.
- Make informed decisions about altitude exposure based on your stage and your data. Awareness isn't avoidance.
What this connects to
Altitude shares deep mechanistic territory with the vascular dysfunction pathway, because what altitude does is essentially stress-test the vascular system's ability to deliver oxygen. The 10,000-Foot Cliff is the deep-dive companion to this article, covering why that altitude is a precise physiological threshold rather than an approximate one. Recognizing Optic Nerve Distress is the practical companion.