Normal Tension Glaucoma: A Category Error
If your pressure looks normal but damage is progressing anyway, the simpler explanation is often that your pressure spikes between appointments — and nobody is looking.
If you've been diagnosed with normal tension glaucoma, the conversation in the exam room probably went something like this.
Your doctor measured your eye pressure. It came back in the normal range. But when they looked at your optic nerve, they saw signs of glaucoma damage anyway. So they explained that some people develop glaucoma even when their pressure looks fine. The diagnosis: normal tension glaucoma. The treatment plan: monitor it, maybe lower the pressure further with drops, come back in three months.
It's worth pausing on that.
Pressure looks fine. Damage is progressing anyway. The standard explanation is that your optic nerve is just unusually sensitive — that something other than pressure must be doing the damage. Maybe blood flow. Maybe genetics. Some people are just unlucky.
That can be true. But for many people who carry this diagnosis, there's a much simpler explanation that doesn't get enough attention.
Pressure isn't normal. It just looks normal at the moments your doctor measures it.
How eye pressure actually behaves
Eye pressure isn't a single steady number. It fluctuates throughout the day, sometimes by a lot. It changes with what you eat, what you drink, what medications you're on, your sleep, your activity, the time of day. Most people's pressure has a pattern — peaks at certain hours, troughs at others, spikes triggered by specific things they consume.
Your ophthalmologist sees a single number. Maybe two, if they take a second reading. Then another number three months later. Maybe four numbers in a year. From those four data points, they're trying to characterize a system that's actually changing minute to minute, hour to hour, day to day.
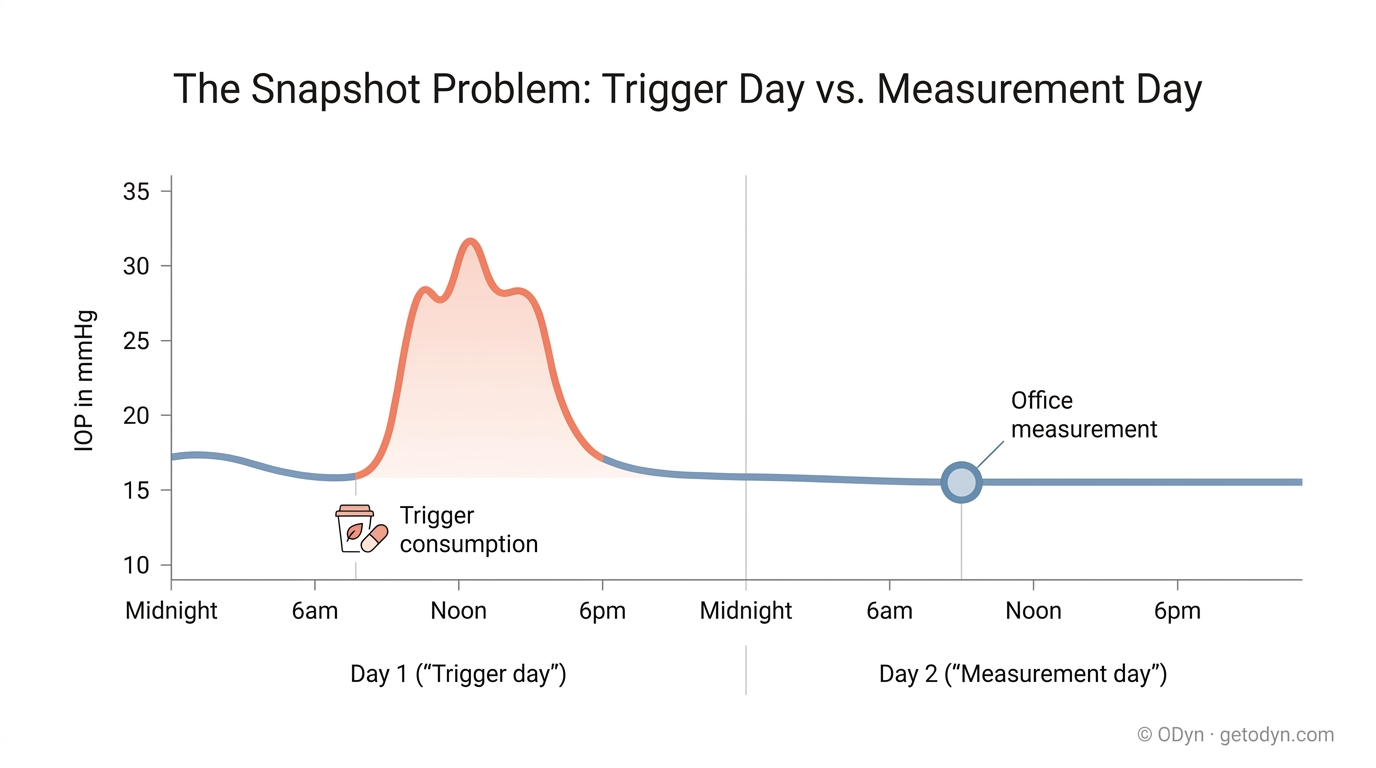
If your pressure spikes for three hours every morning after a particular dietary trigger, and then settles back to normal by your 10 a.m. appointment — your ophthalmologist will never see it. Your file will say your pressure is fine. And technically, at 10 a.m. on the day they measured, it was. But the damage isn't being done at 10 a.m. It's being done at 7 a.m., every morning, and nobody knows.
The gap, not a misdiagnosis
This is the gap. Not a misdiagnosis. Not a failure of your doctor. Just a fundamental limitation of trying to measure something this dynamic four times a year.
And it matters because the spikes that get missed in the exam room are often the most controllable ones. They're frequently driven by something you're eating, drinking, or taking — something you could change tomorrow if you knew it was the cause. But you can't change what you don't know about. And four data points a year aren't enough to find it.
How home tonometry changes the equation
A home tonometer lets you measure your own eye pressure. Multiple times a day. On your own schedule. In your own environment. It's not a replacement for your ophthalmologist — it's the missing layer of data underneath their care.
When you can take ten or fifteen readings a week instead of four a year, the picture changes completely. You start to see your actual pressure pattern — the daily peaks, the typical baseline, the spikes that show up after specific foods or medications. You stop guessing about whether your pressure is "really" normal and start knowing.
For someone diagnosed with normal tension glaucoma, that data is especially valuable. Because if your pressure is actually spiking, and those spikes are driving your damage, that's one of the most actionable forms of glaucoma you can have. The triggers are identifiable. The behaviors are changeable. The progression can be slowed or stopped much more directly than if you assume nothing about your pressure can be changed.
But you have to know.
Either-way framing
We're not suggesting your diagnosis is wrong. Some people genuinely do develop glaucoma that progresses at low pressure — the mechanism is real, and we'll cover it in the piece on vascular dysfunction. What we are suggesting is that for many people who carry the label, the question of whether their pressure is actually "normal" between visits has never really been answered. Home measurement is how you answer it.
If the answer turns out to be "yes, my pressure really is steady at a low level, all day, every day" — that's important information. It tells you the standard pressure-lowering approach has limited room to work, and other interventions deserve more focus.
If the answer turns out to be "actually, my pressure spikes for hours at a time and I never knew" — that's a much bigger finding. Because now you have something specific to work on, and the leverage to slow or stop your progression is dramatically higher than you thought.
Either way, you've moved from guessing to knowing. That's what home tonometry gives you.
In our equipment guide, we'll cover the home tonometers we recommend and how to choose between them. In a separate piece on technique, we'll cover how to take readings that are reliable enough to act on. But the case for home tonometry starts here — especially if you've been told your pressure is "normal" and you're watching damage progress anyway.
That's a question worth answering for yourself.