The Ratchet Effect: How Vision Loss Actually Happens
Glaucoma damage isn't a gradual fade — it's discrete, irreversible events driven by oxygen disruption to the optic nerve.
Most people think glaucoma is a slow erosion of vision. A gradual fade, like an old photograph losing its color over decades.
It isn't.
Glaucoma damages vision in discrete events. Small, often invisible in the moment they happen — but each one permanent. They don't reverse. They don't heal. Each event is a click forward on a ratchet that only turns one direction.

That's the central thing to understand. Once you see it, almost everything about how this disease should be managed changes.
What's actually being damaged
The light-sensing cells at the back of your eye — the retinal ganglion cells, or RGCs — work a lot like the sensor in a digital camera. The eyeball is the lens. The RGCs are the sensor. Together, they convert light into the signals your brain assembles into vision.
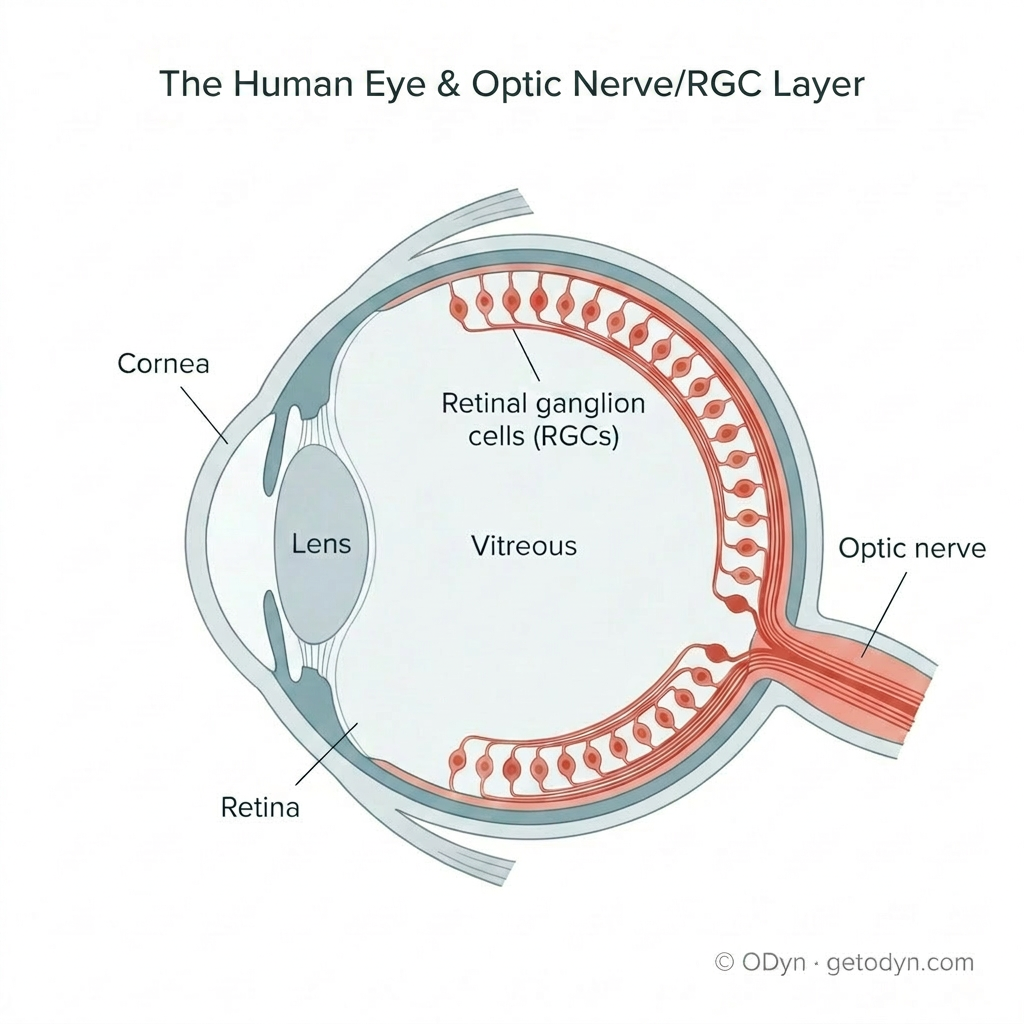
And like any sensor, those cells need power. In this case, that power is oxygen — a constant, reliable supply of oxygen-rich blood reaching every part of the retina and the optic nerve behind it.
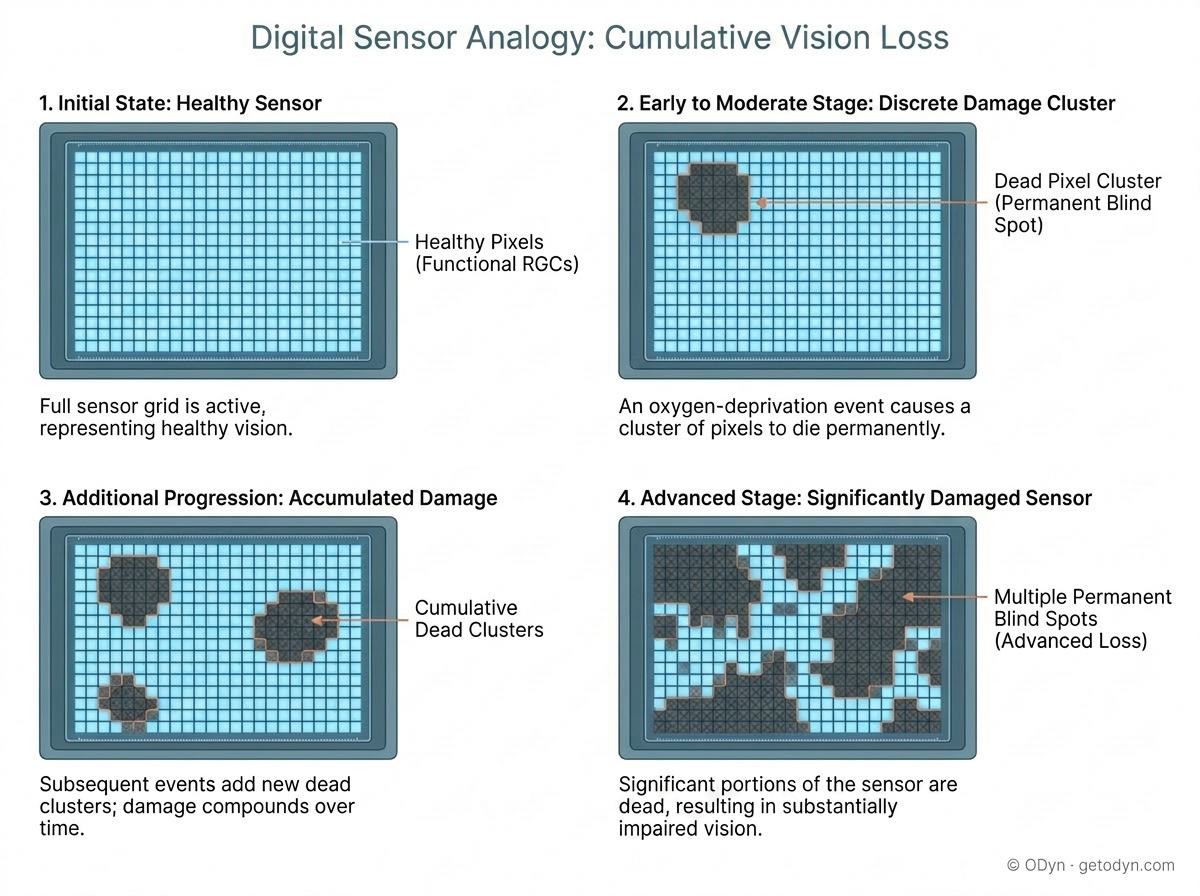
When that supply gets interrupted, even briefly, sections of that sensor start to die. And here's the part that matters: those cells don't come back. The pixels are gone. The blind spot they leave is permanent.
That's the mechanism behind the ratchet. Each oxygen-deprivation event kills another patch of the sensor. The damage accumulates. And over time, those small, scattered blind spots grow into the visible vision loss that defines progressed glaucoma.
A grey zone before death
There's an important nuance. Cells don't always go from healthy to dead in a single step. Some enter a kind of grey zone first — damaged, energy-starved, no longer functioning normally, but not yet beyond recovery. Research has shown that retinal ganglion cells can enter what some scientists describe as a "comatose" state before they die. If the underlying stress is relieved quickly enough, and the cell still has the metabolic resources to repair itself, some of those cells can come back online.
That's not a promise that lost vision returns. Cells that have already died are gone. But it does mean this: when you've just been through a damaging event, fast action matters. Some of what looks like new vision loss may still be salvageable if you can identify the cause and stop it quickly.
The three pathways that disrupt oxygen
What disrupts the oxygen supply? There are three primary pathways, and we'll cover each in depth in its own piece. Here's the framework.
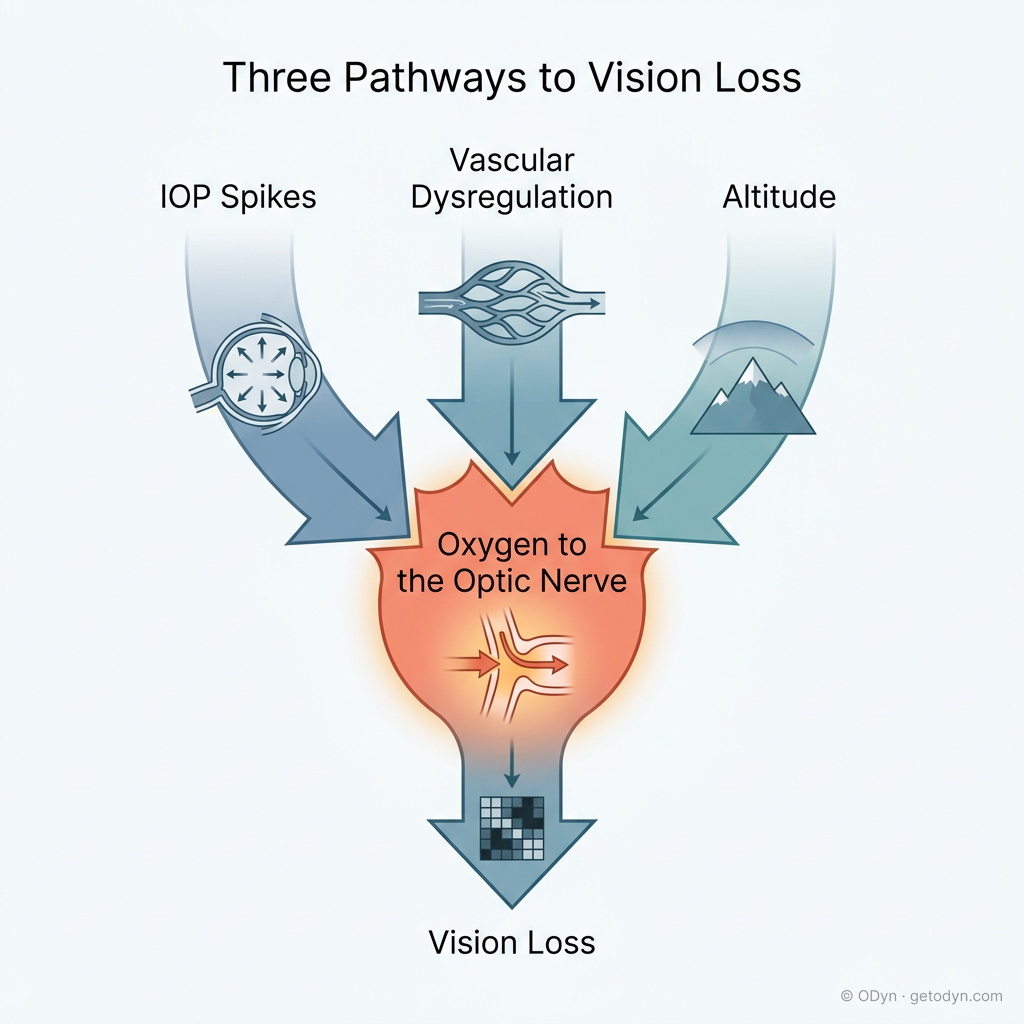
The first pathway is intraocular pressure spikes — IOP spikes. Sudden, sharp increases in the pressure inside your eye. When that pressure rises, it pushes against a structure at the back of the eye called the lamina cribrosa, which is essentially a meshwork the optic nerve fibers pass through. The pressure pinches the small blood vessels feeding those fibers, and the RGCs they support begin to lose their oxygen supply. This is also associated with the cupping at the optic nerve head that an ophthalmologist looks for during an exam.
Here's the part most people don't realize: a spike doesn't have to last for days to cause damage. A few hours is enough. And we believe most spikes, in most people, last only a few hours within a single day — which is precisely why an in-office pressure check, taken once a quarter, almost always misses them.
The second pathway is vascular dysregulation — when the blood vessels supplying the optic nerve fail to deliver oxygen reliably, even at normal eye pressure. Some people are inherently prone to this. But it can also be made worse, sometimes counterintuitively. For example, a supplement like ginkgo biloba is often taken specifically because it dilates blood vessels. The problem is that it dilates blood vessels everywhere — and the body's overall response can actually pull blood away from the optic nerve, where it's needed most.
The third pathway is altitude — and this one becomes much easier to understand once you see oxygen as the root variable. At higher elevations, the air carries less oxygen, and the lower atmospheric pressure also reduces how efficiently your blood absorbs what's available. Both effects reduce the oxygen reaching the optic nerve. Even a perfectly healthy vascular system is operating on a thinner margin at altitude. A compromised system can be pushed past its limit.
How damage compounds
Each time damage occurs, it doesn't just kill cells. It weakens the system's ability to protect itself from the next event. The lamina cribrosa can deform. Blood vessels can be permanently impaired. The optic nerve's ability to autoregulate its own oxygen supply — to compensate when conditions get harder — can be reduced.
Which means the threshold for future damage drops. New pathways for harm open up. The disease becomes easier for itself to progress.
Consider this scenario, drawn from real patient patterns. A person is taking a prescribed medication that, as a side effect, raises eye pressure — and because the medication is taken daily and accumulates in the system, that elevation is sustained over days, not just a few hours at a time. Independently, they begin using a daily nutritional supplement that contains a stack of stimulants — not advertised as such, and not always recognizable as stimulants on the ingredient panel — with each dose driving a sharp 6-to-8-hour pressure spike. Each trigger alone is doing damage. The combination compounds it. And because neither cause is recognized, neither is addressed.
When pressure is sustained at that elevated level for a prolonged period, the small blood vessels feeding the optic nerve are compressed against the surrounding tissue. Compressed long enough, those vessels can deform — their structural integrity changes. And vessels that have lost some structural integrity lose part of their ability to expand and contract on demand. That ability to flex is exactly how blood vessels autoregulate oxygen delivery as conditions change.
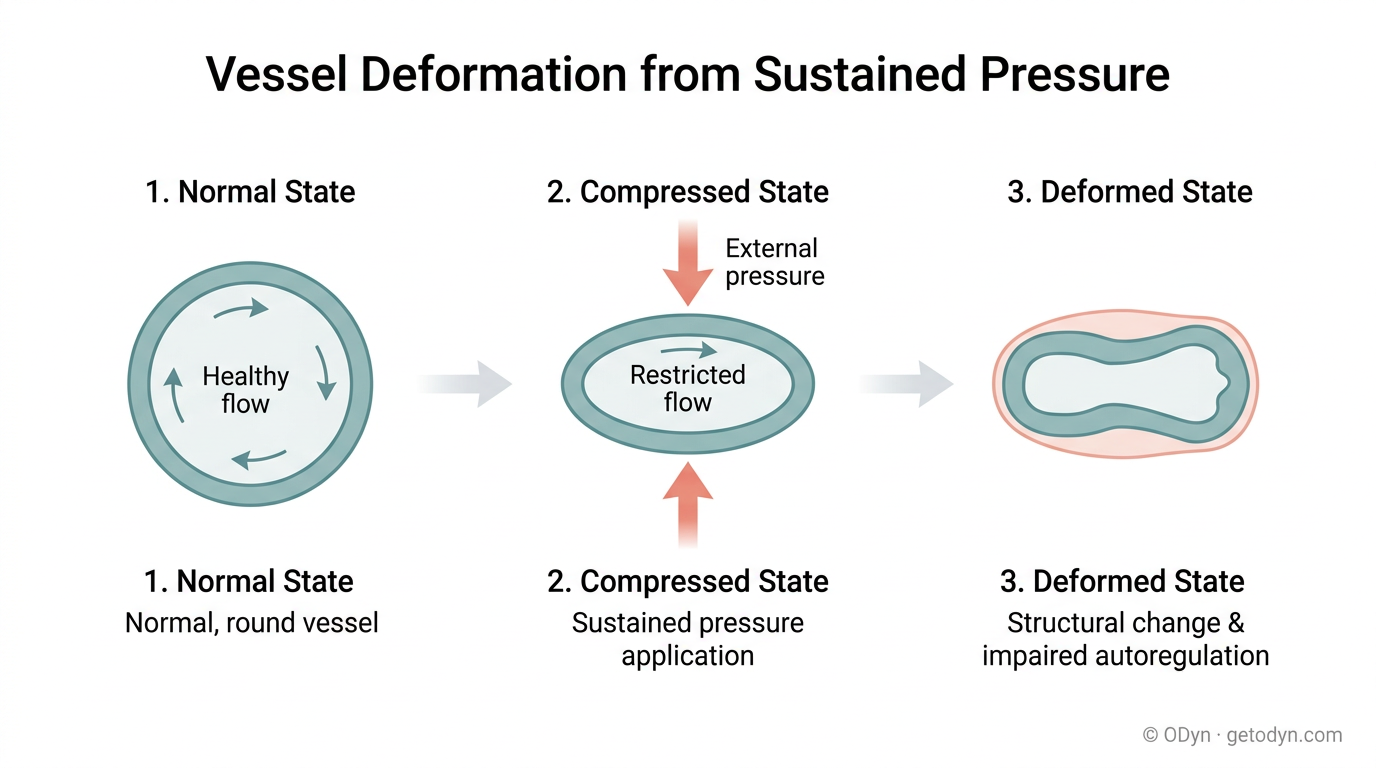
So when this person eventually exerts themselves — particularly at altitude, where the oxygen baseline is already lower — that eye can no longer ramp up its oxygen delivery the way a healthy system would. It drops into a hypoxic state it would have weathered easily before. Each episode is small. Maybe undetectable that day. But the damage compounds. A year later: even more noticeable vision change.
Two ways the optic nerve is harmed
A note on timing. The structural damage to vessels themselves comes from sustained pressure over days, not hours. The earlier point still stands — even brief spikes can kill cells through acute oxygen deprivation. But sustained pressure is what reshapes the underlying machinery and creates new vulnerabilities for the future. Both matter. They damage in different ways.
Why early action matters most
If you've been recently diagnosed, or you're in the early stages, you are at the point where prevention has the highest leverage. The pathways for future damage are still narrow. The system still has its compensating mechanisms intact. Identifying what triggers your spikes — and stopping those triggers — has the most dramatic impact at this stage.
The longer the disease progresses without intervention, the more vectors open up, the more compounding takes hold, and the more difficult management becomes. That's not a reason to despair if you're further along — meaningful prevention is available at every stage. It's a reason to act early if you can.
The ratchet only turns one way. But you have control over how often it clicks.
In the articles that follow, we'll go deeper into each of the three pathways — pressure spikes, vascular dysregulation, and altitude — and into the practical methods you can use to identify what's driving your own progression.