How to Identify What Caused Your Spike
The practical methodology — establish baseline, build cleared list, isolate outliers, confirm by removal, substitute clean alternatives. Most triggers are findable in weeks, not years.
Once you have a home tonometer and you start taking regular measurements, identifying what's causing your IOP spikes is much more straightforward than most patients expect. For dietary triggers especially, the work isn't detective work — it's just observation, structured the right way.
This article walks through that methodology. The goal is that within a few weeks of starting regular measurement you'll have a clear picture of your baseline, and within a few months you'll have a working "cleared" list of your regular items, your primary triggers identified and removed, and a workable approach for catching any new outliers as they show up.
The initial measurement period
When someone first gets a home tonometer, the ideal pattern is frequent measurement — on average every 2 to 4 waking hours, plus one reading just before bed and one shortly after waking. If you happen to wake up in the middle of the night and find yourself lying there for a while, take advantage of the opportunity to measure. Don't force a wake-up to do it; just capture the data when life provides the chance.
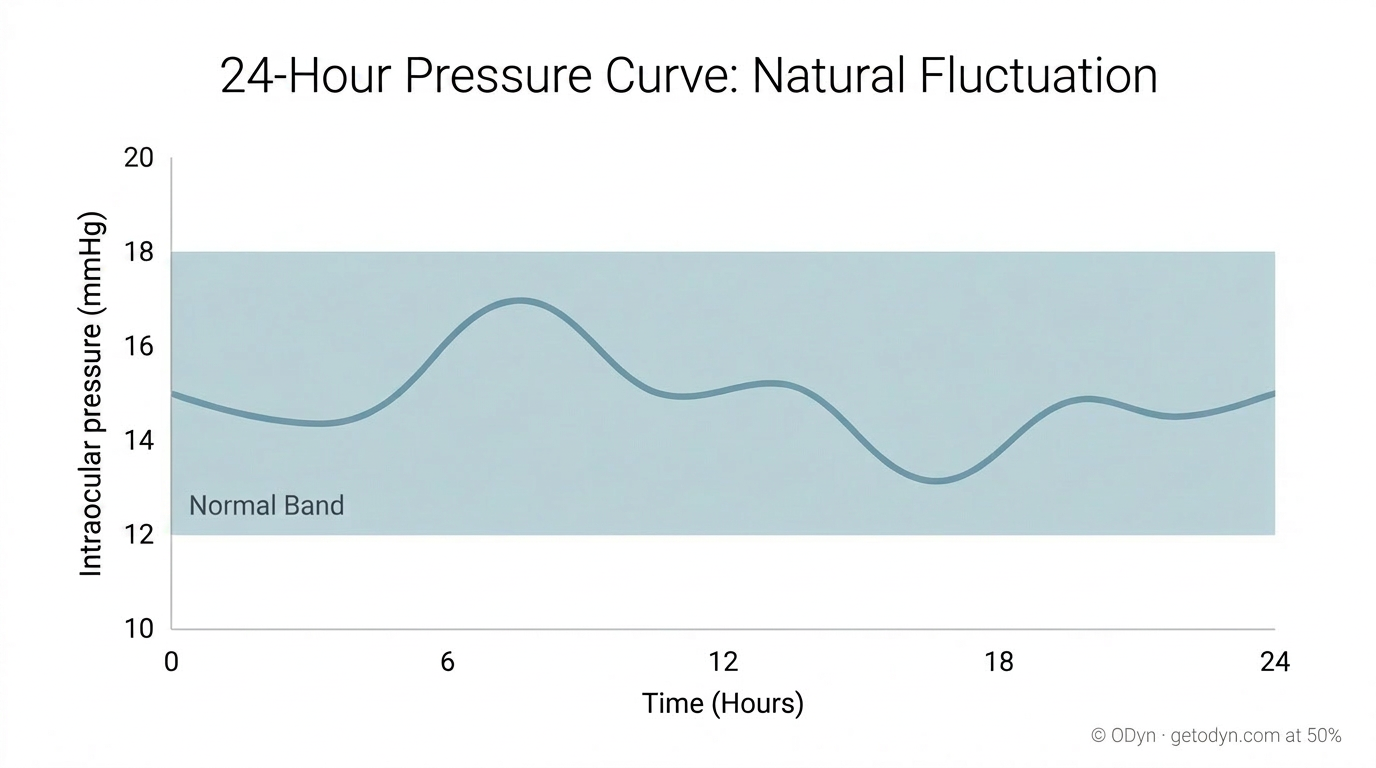
Frequent measurement in the early days is what reveals your baseline. A baseline isn't a single number — it's a pattern. You'll see what your typical morning reading looks like, how it shifts after meals, where it tends to sit in the afternoon and evening, and what your low and high points are across a normal day.
Establishing a clean baseline
ODyn recommends avoiding caffeine and all known stimulants and energy supplements for the first week or so of measurement. The point isn't to declare these products bad — for many patients, the eventual answer will be that some of them are fine. The point is to read your IOP curve with as little noise as possible at the start, so you have a clean reference to compare everything else against.
During this period, ideally, your IOP baseline lands in the range your doctor has targeted. If it doesn't — if your baseline itself is elevated even with stimulants removed — that's an important finding and warrants a conversation with your ophthalmologist. The baseline measurement period isn't only about preparing for trigger identification; it's also about confirming that your underlying pressure control is where it should be.
While you're measuring, pay light attention to what you're eating and drinking. You don't need to track every detail yet. The most important observation in this first period is the absence of spikes during ordinary consumption — because that's how you start building a list of items that aren't problems.
A note on confounders during this period. Rapid intake of large volumes of water can transiently elevate IOP — this is well-documented in glaucoma literature and is the basis of the clinical "water drinking test." If you see a measurement variation shortly after chugging a large glass of water, that's likely the cause and isn't reflective of any dietary trigger. Sip rather than gulp during the baseline period to keep the data clean.
Building your "cleared" list
This is the central insight of the methodology, and the reason dietary trigger identification is much more tractable than it first sounds: most foods and drinks don't significantly affect IOP for most people.
If you've consumed something — caffeine and stimulants aside, during the clean baseline period — and your subsequent measurements stay in your normal range, you can typically count that item as cleared. Even more so once you've consumed it several times across different days with no IOP impact. Cleared items become the foundation against which outliers stand out.
It's worth keeping a mental or written list of what you've cleared. Over the first few weeks, this list grows steadily. Most of what you eat ends up on it. That growing list is what makes everything that follows easy — when 90% of your normal diet is on the cleared list, anything new or unusual that gets ingested becomes much easier to isolate when a spike appears.
Avoiding coverage gaps
The methodology depends on actually measuring during the window when a trigger could be producing a spike. It's possible — and surprisingly common — to consume a serious trigger regularly for months or longer without ever catching it, simply because the timing of your measurements never overlaps with the spike it produces.
A common pattern: someone makes a smoothie or breakfast item at 7:30 in the morning, leaves the house, and isn't back to take another reading until mid-afternoon. By that point, even a 7-to-8-hour spike has largely resolved. What they may notice — if anything — is a slightly elevated reading at 3 or 4pm that comes down over the next hour, which gets written off as ordinary variation. What they're actually seeing is the back end of a major spike resolving. The peak, the duration, and the actual damage being done all stay invisible because the measurement schedule and the trigger window never overlap.
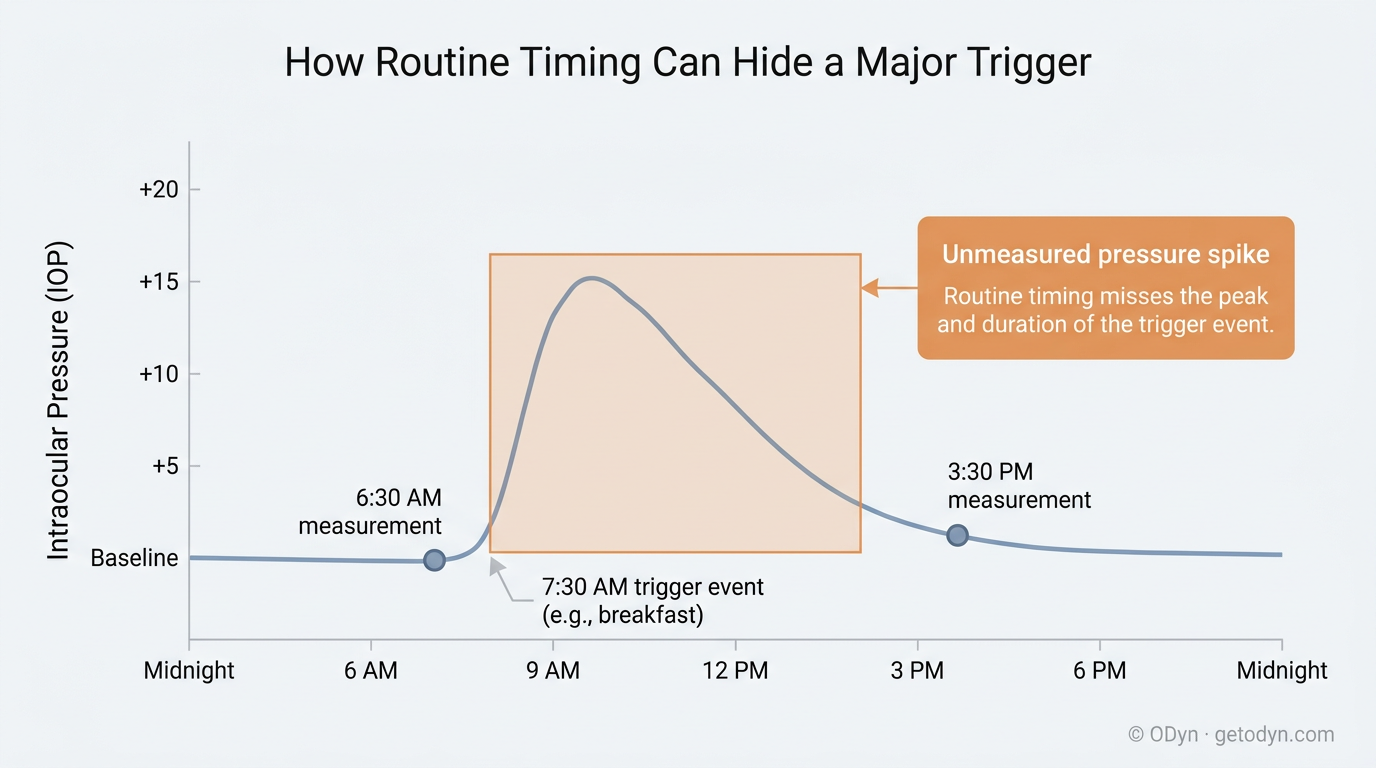
This kind of coverage gap can persist for a year or longer in patients who are otherwise measuring conscientiously. It's a particular risk for items consumed at the same time every day, where a routine timing coincidence (you leave the house at the same time, you eat the same breakfast) hides the full spike pattern from the measurement record. By the time the gap is identified, real visual field progression may already have occurred from a trigger the patient never realized they had.
The defense is simple in principle and worth doing deliberately: make sure you've measured your IOP at least once within a few hours of consuming every regularly ingested item, no matter how innocuous it seems. That includes the morning smoothie, the lunch staple, the afternoon snack, the supplement you take with dinner — each of them needs to have been verified by direct measurement at least once during the post-consumption window. Items consumed irregularly or episodically count too: anything you ingest, even infrequently, eventually deserves a measurement check during its post-consumption window.
This is a one-time exercise per item, not a permanent burden. Once you've measured within the spike window for a given item and confirmed no impact, that item joins the cleared list and routine measurement can return to its normal cadence. But until you've done that initial verification, the item's status is unverified, not cleared — even if you've eaten it for years and feel certain it's fine.
The risk to watch for is reducing measurement frequency too early, before you've completed this coverage check. Confidence based on incomplete coverage isn't real confidence — it's untested assumption. Stay deliberately rigorous in the first several weeks to months, until you can honestly say you've directly measured around every regularly consumed item in your diet.
Reintroducing caffeine and stimulants methodically
Once you have a clean baseline, if there are caffeinated or stimulant products you'd prefer to keep consuming, you can resume them gradually — but methodically. The key rule: avoid consuming two or more stimulant products within a 6 to 8 hour window.
The reason is signal clarity. Stimulants and caffeine almost always produce some IOP impact. The question worth answering is how much, for each specific product. If you ingest product A and product B within an hour of each other and you see a spike, you can't tell which one caused it, or how much each contributed. By spacing them out, you give each one a clean window in which its effect is readable.
There is one thing that consuming multiple items together can tell you: the absence of triggers. If you ingest products A, B, and C within a two-hour span and no elevation occurs, all three are reasonably cleared.
The complication is specific to caffeine and stimulants. Most ordinary foods don't impact IOP, so when a single suspect among several normal items causes a spike, the lone outlier is usually identifiable. But stimulants are different — most of them produce some impact. Consume two or three together and you'll likely see a spike, but you'll have lost the ability to cleanly attribute how much of the impact came from each. Spacing them gives you a clean magnitude read on each, which matters because the action you take depends on it: a product producing a +3 spike sits in very different territory from one producing a +12.
If the combination is your normal real-life consumption pattern — an espresso plus a pre-workout supplement, for instance — there's practical value in eventually measuring the aggregated impact, since that's the actual exposure you're operating under. But you'll still want clean reads of each one individually first. Combined effects are usually close to the sum of the individual impacts, and it's much more useful to know that one of the three is the major contributor while the others are minor than to see only the aggregate.
Many patients find that the elevation produced by their preferred stimulant is moderate, the benefit-to-risk trade-off acceptable, and they continue using it. Others find the elevation more significant than they're willing to accept and substitute or eliminate. Both are reasonable responses; the methodology gives you the information needed to make the call.
What counts as a meaningful spike
Not every fluctuation requires action. But it's worth being clear about thresholds.
For most patients managing NTG or POAG, the following framework is a useful general guide:
- +5 to +8 above baseline is a caution zone. Worth additional measurements over the next several hours to track recovery, and worth noting the context for later pattern matching.
- +9 or more above baseline should be considered progression-prone. Spikes in this range, repeated regularly, are likely contributing to ongoing damage.
- +14 or more above baseline, or any spike that pushes above 20 mmHg, should be treated as almost certainly causing progression. Acute visual field degradation can occur with IOPs in the mid-20s. With your vision as your primary sensory input, you want a meaningful buffer below that range.
These are general thresholds. Your ophthalmologist may set more conservative targets depending on your specific disease stage, optic nerve integrity, and treatment plan — and for NTG patients with documented damage at "normal" pressures, even smaller absolute changes can matter. The principle is the same regardless: spikes of meaningful magnitude warrant identification and removal of the cause.
It's also worth knowing that visual symptoms — the kind of optic nerve distress signals discussed in the previous article — are an additional confirming signal that an event occurred. If a measured spike is accompanied by haziness, gray-outs, or graduated visual field changes, the case for treating that event as a real trigger event rather than a measurement anomaly becomes considerably stronger.
Magnitude and duration both matter
A spike isn't just a number — it has a shape. A +9 spike that resolves in a few hours and a +9 spike that lasts several hours or more are very different events. Both cause progression. The longer one causes much more.
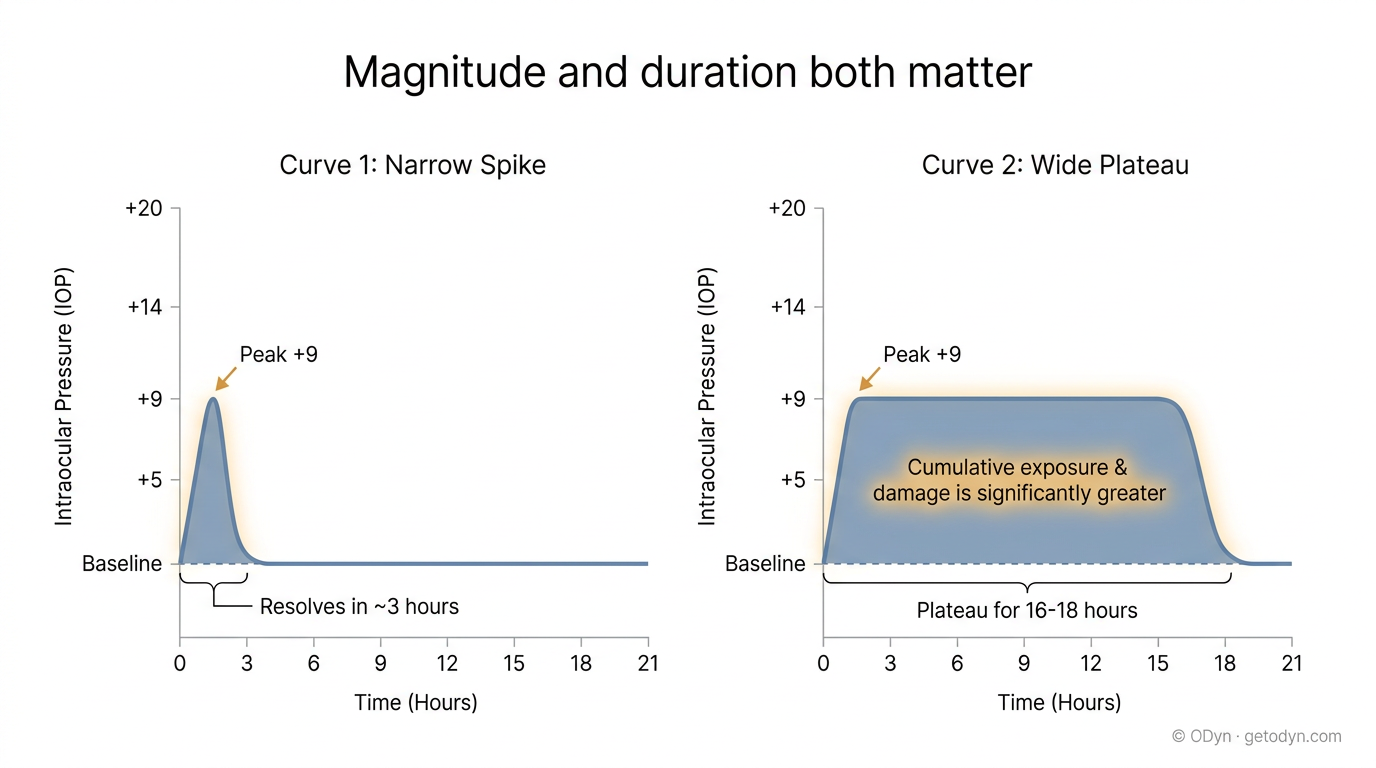
Different triggers produce different durations. Some products cause a 3-to-4-hour elevation; others cause spikes that persist for 7 to 8 hours or longer. Two triggers might produce the same peak magnitude but very different cumulative exposure — which means very different cumulative damage.
Two practical implications for how you measure.
Catch the peak. Take a measurement within roughly 2 hours of consuming any new or uncleared item. This gives you the best chance of capturing the spike at or near its peak. Wait too long and you may catch the back end of the curve, where the reading has already begun to decline — leading you to conclude the impact was milder than it actually was, or to miss the event entirely.
Track the resolution. Once you've detected a spike, don't stop measuring. Continue at roughly 30-minute intervals until the reading returns to baseline. This tells you the full duration, which informs both the severity of the event and how aggressively to act on the trigger. ODyn includes a guided spike-management workflow with timed measurement reminders to make this routine — the methodology is detailed in the Using ODyn section.
A point worth being explicit about: even brief spikes — a 1-to-2-hour event — are long enough to cause progression. The damage from any single short event may be too small to detect on a visual field test in early-stage glaucoma. But spikes don't happen in isolation. They happen repeatedly, often invisibly, and the cumulative damage compounds. A meaningful share of the "unexplained" disease progression in patients with otherwise good adherence is caused by exactly this pattern: small individual events, dismissed as minor, accumulating over months and years.
The goal is to interrupt that compounding before the disease progresses from early to moderate, or moderate to severe. As covered in Vascular Dysfunction, each step of progression opens additional pathways for further progression — vascular dysregulation worsens, the optic nerve's reserve narrows, the threshold for triggering an event drops. Stopping spikes in early-stage disease is qualitatively different from stopping them later. With consistent diligence beginning early, it's often possible to substantially slow or arrest progression by depriving it of the events that drive it forward.
Identifying outliers when a spike occurs
Once you've built a meaningful cleared list, the methodology becomes simple. If 90% of your diet is cleared and one day you see a spike of 8 to 12 points or more within an hour or two of a meal or drink, the question writes itself: what was new, or uncleared, in that meal?
That's the assignment. Identify the uncleared but ingested items.
When you have your suspects, photograph each product clearly — the front of the package, the full ingredient panel, and ideally the UPC barcode if available — and upload them to ODyn as trigger candidates. ODyn processes the ingredients and surfaces whether there's a single likely culprit, or a combination of two or more products whose ingredients stack in a way that explains the spike. The output also includes the underlying reason: why the specific ingredient or combination is implicated, including the molecular mechanism and the relevant physiology.
This is where structured ingredient analysis matters. A whole-greens supplement looks innocuous on the front label. The ingredient list, examined at the molecular level, may show a stack of stimulants that no patient would ever assemble individually but that the product combines as a feature rather than a flaw. Without ingredient-level analysis, the suspect stays unrecognizable. With it, the smoking gun becomes obvious.
Confirming a trigger
Confirmation is the part that sounds more involved than it usually needs to be.
Strict scientific positive confirmation would mean ingesting the suspected trigger again, in isolation, and re-inducing the spike to verify. This isn't recommended. The whole point of identifying triggers is to avoid spikes; deliberately re-inducing one risks additional progression.
A better approach is negative confirmation: remove the suspected product from your routine and consume the rest of the meal or context exactly as before. If everything else is on your cleared list and the spike doesn't recur, that's strong evidence that the removed item was the cause — without re-triggering the event.
ODyn also reduces the confirmation threshold by aggregation. When the same product or ingredient stack is associated with spikes across many users, the evidence accumulates without any single user needing to take the risk of re-triggering. The pattern becomes statistically clear from the population, and the individual user can act on the finding without further self-testing.
Removing a trigger — and what's actually being removed
Once you've identified a trigger that produces a meaningful spike, the action is straightforward: remove it permanently.
This is usually easier than it sounds, for two reasons.
First, recall that most products don't trigger spikes. The few that do tend to be non-essential — supplements, specific processed foods, certain beverages — and are usually easy to substitute or eliminate without significant lifestyle impact.
Second, when a product is identified as a trigger, it's almost always the specific formulation that's the problem, not the entire category. ODyn's report identifies the specific ingredient or combination contributing to the spike, which means you can find a different product in the same category without that ingredient stack and continue consuming the category without issue.
A couple of concrete examples illustrate how this typically plays out.
Example one: veggie sausage. A patient identifies that their morning frozen veggie sausage is consistently producing a 10-point IOP spike. The ODyn ingredient analysis flags the cause as MSG plus several sodium-based flavor enhancers stacked in the same product. The fix isn't to give up veggie sausage as a category; it's to find a different brand whose ingredient panel doesn't contain that specific stack. A clean alternative becomes the new staple. The spike disappears.
Example two: morning smoothie. A patient's homemade smoothie — fruits, supplements, protein powder, organic juices — is producing repeated mid-morning spikes. The ODyn analysis works through each ingredient panel and flags an unassuming whole-greens powder as the smoking gun. The greens powder, examined molecularly, contains a stack of stimulants that's silently spiking IOP by 10 to 15 points or more. The fix is to replace that one powder with a clean alternative. The smoothie continues; the spike resolves.
In both cases, the methodology came together as: regular measurement, an established cleared baseline, a flagged event, ingredient analysis, and a substitution. No years-long investigation. Often a matter of weeks from first spike to identified cause to clean removal.
Pre-emptive scanning of substitutes
Just as ODyn can analyze ingredient labels after a spike to identify the culprit, it can also scan candidate substitutes before you consume them. If you've identified that the trigger in your greens powder is a specific stimulant stack, you can scan a candidate replacement powder before adding it to your routine to confirm it doesn't contain the same combination. This preempts a second cycle of spike-and-investigate.
This is one of the most valuable uses of the platform once you understand your own triggers — it shifts trigger management from reactive to proactive. New products get cleared before they enter your diet, not after.
Ongoing monitoring
Trigger identification isn't a one-time exercise.
Food and supplement manufacturers reformulate their products. A staple that's been on your cleared list for months may show up one day with a "New & Improved" label, and the new formulation may include components that weren't there before. Long-term routine tonometer checks catch these reformulations early; targeted measurement around any product newly marked as reformulated catches them at first introduction.
Your own physiology can also shift. New medications, new health conditions, age, hormonal changes, or seasonal factors can move your baseline or change which products affect you. Ongoing measurement keeps the picture current.
The work doesn't stay equally intensive forever. The first weeks to months of measurement are the most demanding — that's when you're building your baseline, completing coverage of your regular items, identifying and removing your initial triggers. After that, diligence shifts from active investigation to something more passive and routine: periodic measurement to confirm continued stability, focused measurement around new products or unusual circumstances, and ongoing alertness for the occasional rogue trigger that slips in. The heavy lift is upfront. The lighter ongoing rhythm that follows is sustainable indefinitely — and necessary, because the system doesn't go fully on autopilot.
A closing observation
For most patients, the practical experience of trigger identification is much less demanding than a description of the methodology might suggest.
Most foods don't trigger spikes. The few that do tend to be specific formulations rather than entire categories. The methodology — establish baseline, build cleared list, isolate outliers, confirm by removal, substitute clean alternatives — runs in the background of normal life once the habit of measurement is established. And the reward is direct: each identified and removed trigger eliminates a recurring source of disease progression and the vascular stress that follows each spike.
Triggers are findable. They're typically sparse. The intensive identification phase ends in months, not years. What follows is lighter — routine measurement, periodic verification, alertness for change — but it's the part that makes the protection durable.